194. BURST FRACTURE -- axial loading (ie, diving ) , retropulsion of bony fragments
into the spinal canal -----> spinal cord compression.
UNSTABLE; neuro deficits
in approx 50%; often misdiagnosed as stable ant. wedge fractures; order CT is
suspicious
2. NEXUS criteria: MILDD (no imaging needed if
no Mtenderness, I, altered L, D
injuries, neuro D).
29. Prox tibial plateau fx: risk for compartment syndrome. Pain with passive ROM (first
sign), last sign is lost pulses (you are screwed). Pressures > 30 mmHg. Remove splint
and ortho to do
fasciotomy.
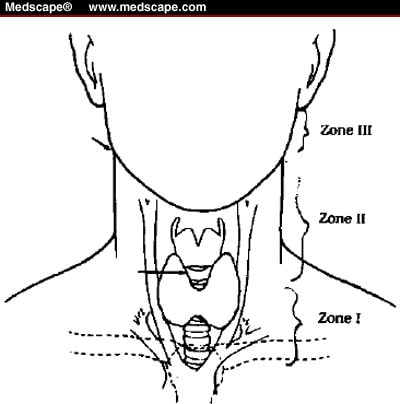
47. Neck injuries: (#255)
Is platysma intact ?? ** if platysma is violated, then immediate surgical consultation is warranted
Zone I (esophageal , tracheal eval, angiogram)
Zone II (esophageal eval with esophogram and esophagoscopy vascular evaluation with angiogram)
Zone III(angio). If trachea is damaged you will know it right away,
*Injuries to the esophagus are notoriously asymptomatic initially --->damage may lead to mediastinitis and neck space infections, so esophagram/oscopy may be done
if stable. Zone II (hard signs then surgically explore)
Zone I = the base of the neck, is demarcated by the thoracic inlet inferiorly and the cricoid cartilage superiorly.
Zone II = encompasses the midportion of the neck and the region from the cricoid cartilage to the angle of the mandible.
Zone III = characterizes the superior aspect of the neck and is bounded by the angle of the mandible and the base of the skull.