Case Study: A 34-year-old woman presents to the ED with a 3-day history of right-sided headache and facial pain. Today, she felt dizziness and burning in her left arm and leg, and she had trouble walking. On exam you note reduced gag reflex and numbness over her R face. What is your diagnosis??
➥WALLENBERG'S SYNDROME (Good Article --------->>>Wallenberg from Medscape Article )
- The classic sign of a brainstem stroke is presence of crossed symptoms: ipsilateral cranial nerve palsy and contralateral hemiplegia (motor weakness) or contralaeral sensory deficit
- in Wallenberg, pateints may present with ipsilateral facial pain (sharp or stabbing) vertigo, headache, limb ataxia, Horner syndrome,
- Contralateral symptoms include loss of pinprick and temperature sensation in the arm and leg
- The lateral medullary syndrome ( Wallenberg or posterior inferior cerebellar artery [PICA] syndrome)
- Most common brainstem stroke
- The loss of pain and temperature sensation on the ipsilateral side of the face and contralateral side of the body is characteristic of this condition
- Other clinical features include intractable hiccups, vertigo, Horner syndrome, nystagmus, dysarthria, dysphagia, and ipsilateral ataxia.
- The blood supply to the medulla is mainly from the vertebral arteries.
- The posterior circulation supplies blood to the brainstem, cerebellum and visual cortex.
- lateral medullary infarctions occur due to involvement of the vertebral artery in 38% of cases. PICA is involved 14%-24% of the time, and both arteries are involved in 26% of cases. No abnormality is found in either vessel only 12%-19% of the time.
- impairment of pain and temperature (ie, spinothalamic) sensation on the right side of the face and the left side of the body. These contralateral findings are characteristic of a right lateral medullary lesion.
- ipsilateral facial pain and numbness
- ipsilateral ataxia (falling to the side of the lesion)
- The patient also had reduced palatal movements and gag reflex on the right side indicative of involvement of the right IX (glossopharyngeal) and X (vagus) cranial nerves. These cranial nerves, as well as the descending sympathetic fibers (patient had a right-sided Horner's sign), are also found in the dorsolateral aspect of the right side of the medulla (Figure 2).
- . The presence of vertigo and right-sided ataxia was due to involvement of the vestibular nucleus and cerebellar pathways (as they pass into the cerebellum through the inferior cerebellar peduncle), respectively, on the right side.
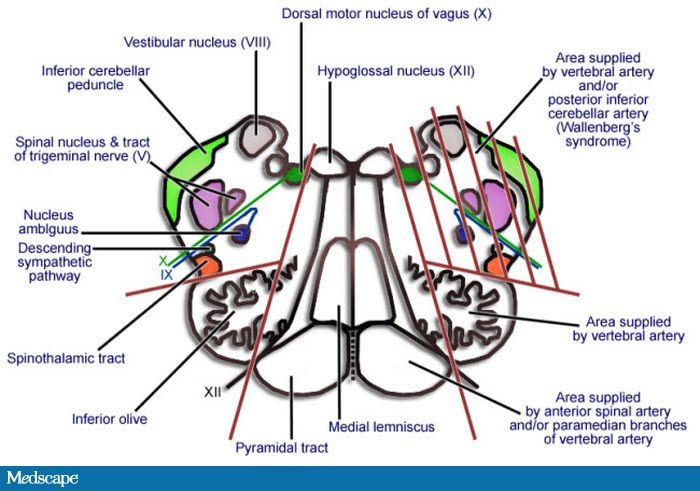
Neurons relaying pain and temperature sensation from the right side of the face synapse in the descending spinal nucleus of the trigeminal nerve, which lies in the dorsolateral aspect of the brainstem (Figure ------------------>>>
Lateral medullary syndrome (Wallenberg syndrome)
This is the commonest of the brain stem strokes. Involvement of the spinothalamic tract results in contralateral loss of pain and temperature sensation below the neck. Involvement of the descending nucleus and tract of V results in loss of pain and temperature sensation on the face ipsilateral to the lesion. Involvement of descending autonomic fibers results in an ipsilateral Horner's syndrome (ptosis, meiosis, and anhidrosis). Involvement of the nucleus ambiguus causes palatal weakness and dysphagia. Involvement of the inferior cerebellar peduncle (restiform body) causes ipsilateral ataxia.

This is the commonest of the brain stem strokes. Involvement of the spinothalamic tract results in contralateral loss of pain and temperature sensation below the neck. Involvement of the descending nucleus and tract of V results in loss of pain and temperature sensation on the face ipsilateral to the lesion. Involvement of descending autonomic fibers results in an ipsilateral Horner's syndrome (ptosis, meiosis, and anhidrosis). Involvement of the nucleus ambiguus causes palatal weakness and dysphagia. Involvement of the inferior cerebellar peduncle (restiform body) causes ipsilateral ataxia.